Keto Blood Lipids That Shocked Doctors: What Rising LDL Really Means for You
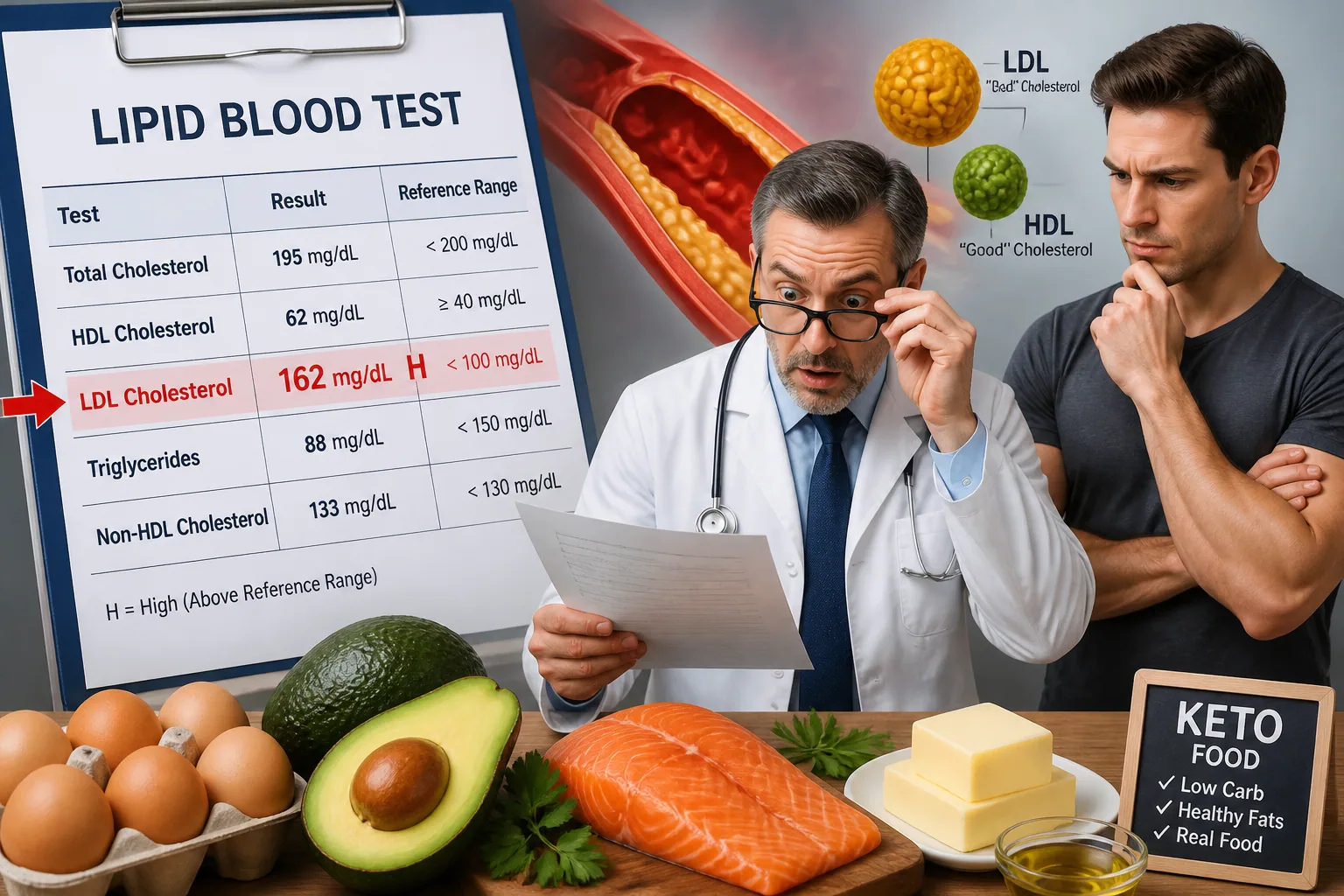
Keto can change the way your body uses fuel, and for some people, it changes blood lipids in a way that looks alarming on paper. The biggest shock is usually LDL cholesterol. On a standard lab report, a high LDL-C number can feel like an obvious warning sign, but keto makes the picture more complicated than that. In some people, especially those who are lean, active, and metabolically healthy, LDL can rise dramatically even while triglycerides stay low and HDL stays high. That is why this topic has become such a debate.
The key question is not whether LDL matters at all. It does. The real issue is how much meaning to give LDL by itself, and whether someone on keto needs a different way to look at risk. To answer that, it helps to understand the newer research on LDL-C, apoB, particle patterns, and plaque, plus the people most likely to see big lipid changes in the first place.
Why Keto-Related LDL Spikes Are Causing So Much Debate
The debate exists because keto often improves several markers that doctors usually love to see. Triglycerides often fall, HDL often rises, blood sugar control often improves, and insulin resistance can improve as well. At the same time, some people see LDL-C soar. That creates a strange lab pattern: the classic risk marker goes up, while many other markers look better than ever.
That mismatch is especially unsettling because the usual story of cardiovascular risk is built around LDL. For decades, higher LDL has been linked to higher risk of atherosclerosis. But keto introduces a group of people whose lipid profile does not behave like the usual metabolic syndrome pattern. They can look healthy, feel healthy, and still have LDL levels that would normally trigger serious concern.
Researchers have started to focus on whether these LDL increases are more of a biochemical curiosity, a temporary adaptation, or a true long-term problem. The answer is still not settled, which is why careful interpretation matters more than panic.
What the Latest Studies Actually Show About Keto and Cholesterol
One of the most important findings in recent research is that keto-related LDL rises are not random. In a large survey of carbohydrate-restricted eaters, LDL-C change was inversely related to BMI, meaning the leaner the person, the bigger the LDL rise tended to be. Lower triglyceride-to-HDL ratios, which usually signal excellent metabolic health, also predicted larger LDL increases. In other words, the people who looked healthiest by many markers were often the ones with the biggest LDL jump. Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC8796252/
A smaller but striking case report described a person in the Lean Mass Hyper-Responder range whose LDL-C rose from 95 to 545 mg/dL while HDL-C climbed above 100 mg/dL and triglycerides stayed around 40 mg/dL. After about 2.5 years, coronary CT angiography showed no detectable calcified or non-calcified plaque in that individual. That does not prove safety for everyone, but it does show why a single LDL number may not tell the whole story in a short time frame. Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC9048595/
More recent work has looked at people with very high LDL on keto and compared them with matched controls from a heart cohort. The KETO Trial and follow-up studies are trying to answer the plaque question more directly, but the data are still early and limited. Some prospective follow-up in LMHR-type participants found modest plaque progression over about one year, with baseline plaque burden appearing to matter more than cumulative LDL exposure in that short window. That is an important clue, but it is not the final word on long-term risk. Source: https://www.medrxiv.org/content/10.64898/2026.01.15.26343955v1.full/
Why LDL Can Rise on Keto, Especially in Lean, Active People
There are several plausible reasons LDL rises on keto. One popular explanation is the lipid energy model, which suggests that when the body is relying heavily on fat for fuel, lipoprotein transport may change to move more lipid through the bloodstream. In lean, active people with low carbohydrate intake and low insulin levels, this effect may be amplified because the body is using and mobilizing more fat overall.
This may help explain why the biggest LDL increases often appear in lower-BMI individuals. A cohort of hyper-responders found average LDL rose by about 245% after roughly 12.3 months on strict keto, then dropped after people stopped keto. The largest percentage increases were seen in people with lower BMI, and a few had LDL receptor variants that could also contribute. Source: https://www.sciencedirect.com/science/article/pii/S2666667723000892
Another study in lean healthy women found LDL-C increases were associated with body composition and thyroid markers such as free T3 and T4, rather than saturated fat intake alone or typical insulin resistance markers. That matters because it suggests LDL changes on keto may sometimes reflect a complex metabolic response, not just one food choice. Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC10768172/
There is also evidence that caloric balance matters. In a small n=1 experiment, LDL-C and apoB increased during caloric restriction and decreased with overfeeding, even though saturated fat intake increased during the overfeeding phase. That points to the possibility that energy availability, not just fat type, can influence lipid response. Source: https://pubmed.ncbi.nlm.nih.gov/35938774/
Meet the Lean Mass Hyper-Responder Phenotype
The Lean Mass Hyper-Responder, or LMHR, has become the most discussed phenotype in the keto lipid debate. It is generally defined as someone on a carbohydrate-restricted diet with LDL-C of at least 200 mg/dL, HDL-C of at least 80 mg/dL, and triglycerides of 70 mg/dL or lower. These are not the usual signs of poor metabolic health. In fact, the pattern is almost the opposite of the classic atherogenic dyslipidemia seen with insulin resistance. Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC8796252/
The LMHR group tends to be lean, often physically active, and frequently displays very low triglycerides, very high HDL, and normal or low insulin resistance markers. That is why this phenotype stands out so much. The issue is that the LDL-C number can be extreme, sometimes far beyond what a clinician expects to see in someone who otherwise looks metabolically fit.
The important takeaway is that LMHR is not a guarantee of safety, and it is not a diagnosis in the formal medical sense. It is a pattern that researchers are using to better understand why some people react so strongly to carbohydrate restriction. If your lipid panel fits this pattern, it is worth looking beyond LDL-C alone and discussing the full picture with a clinician.
LDL, ApoB, HDL, Triglycerides, and Particle Size: What Matters Most?
LDL-C measures how much cholesterol is carried inside LDL particles. ApoB is different. It reflects the number of atherogenic particles, including LDL and some related particles. Many clinicians consider apoB a stronger marker of risk than LDL-C alone because it counts the number of particles that can enter the artery wall.
HDL and triglycerides are also useful, not because they cancel out LDL risk, but because they help show the broader metabolic context. High HDL and low triglycerides often go with better insulin sensitivity and less metabolic dysfunction. On keto, that pattern is common. The problem is that LDL-C can still be very high even in that favorable context.
Particle size is often discussed in these conversations too. Bigger LDL particles are sometimes seen as less worrisome than smaller, denser LDL particles, but particle size alone is not a complete shield. If apoB is high, the overall number of atherogenic particles is still a concern. That is why many lipid specialists now prefer to look at apoB, non-HDL cholesterol, triglycerides, HDL, and possibly Lp(a) alongside LDL-C, rather than relying on one value alone.
In practice, non-HDL cholesterol can also be helpful because it captures all cholesterol carried by atherogenic particles. If your LDL-C is high on keto, but apoB and non-HDL are also high, concern is usually greater than if LDL-C rises modestly while the rest of the metabolic picture is exceptionally favorable. The challenge is that the evidence base for keto-specific risk interpretation is still evolving.
Does High LDL on Keto Mean Higher Plaque or Immediate Danger?
Not necessarily immediate danger, but not no risk either. That is the honest answer. The most interesting recent studies suggest that very high LDL in LMHR-like people does not always map neatly to short-term plaque progression, especially when baseline plaque burden is low. In some follow-up data, plaque progression over roughly one year was modest, and baseline plaque measures seemed more predictive than cumulative LDL-C exposure in that period. Source: https://www.medrxiv.org/content/10.64898/2026.01.15.26343955v1.full/
The case report showing no detectable plaque after years of extreme LDL is also frequently cited because it challenges the assumption that a very high LDL number always means an equal level of near-term danger. But a single case is not enough to rewrite cardiovascular biology. It simply shows that the relationship between LDL and plaque can be more nuanced than the lab report suggests. Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC9048595/
What we can say is that plaque does not seem to appear overnight just because LDL rises on keto. That is reassuring in the short term. What we cannot say is that long-term exposure to very high LDL is harmless, especially across decades. That uncertainty is exactly why ongoing monitoring and individualized care matter.
What We Know About Short-Term Findings vs Long-Term Risk
Short-term findings are encouraging but incomplete. Many keto hyper-responders appear to have minimal plaque progression over periods measured in months to about a year, particularly when baseline plaque is low. That suggests the risk story may not be identical for every person with a high LDL-C reading. But atherosclerosis is a long disease process, and a year is not long enough to settle the question.
Long-term risk remains debated because the key questions are still unanswered. Do LMHRs eventually accumulate plaque at the same rate as others with similarly high LDL? Does high apoB matter more than LDL-C in this group? Are there protective features in the low insulin, low triglyceride state that change the meaning of LDL exposure? Researchers are still working through these issues.
For now, the safest approach is to treat high LDL on keto as a signal to investigate, not as an automatic reason to abandon the diet or ignore the result. That means checking the broader context, tracking trends over time, and watching for signs of inherited lipid disorders or other hidden risk factors.
Who Should Be More Cautious Before or During Keto
Some people deserve extra caution before making keto a long-term diet. This includes people with a family history of early heart disease, known familial hypercholesterolemia, previous coronary calcium, prior cardiovascular events, elevated Lp(a), type 1 diabetes, or strong genetic lipid disorders. If LDL rises sharply in any of these settings, the threshold for concern should be lower.
People who are already lean, very active, and metabolically healthy may be the most likely to develop an LMHR pattern. That does not mean they are doomed to have bad outcomes, but it does mean they are the group in which lab results can become especially extreme. If you already know that your LDL tends to run high, keto may push it even higher.
Anyone considering keto for medical reasons should ideally know their starting numbers first, including LDL-C, apoB, non-HDL cholesterol, triglycerides, HDL, A1c, and possibly thyroid markers. That baseline makes it much easier to spot meaningful changes later.
How to Monitor Lipids Safely While Staying in Ketosis
If you want to stay in ketosis but reduce uncertainty, the answer is monitoring. A practical approach is to check a full lipid panel after you have been stable on keto long enough for your numbers to settle, then repeat it as needed with your clinician. If LDL rises sharply, add apoB and non-HDL cholesterol if they were not already included. Consider Lp(a) once if it has never been measured, because it is largely genetic and can meaningfully change overall risk interpretation.
It can also help to track body weight, waist circumference, blood pressure, fasting glucose, fasting insulin if available, and thyroid function if symptoms or major lipid changes appear. The point is to see whether the lipid shift comes with broad metabolic improvement or whether it is happening in a less favorable context.
If you are a keto shopper trying to keep the diet practical while paying attention to your health, a tool like Keeto - Keto Made Easy can make day-to-day food decisions easier. It lets you scan products, check net carbs, and stay within your carb budget without constant guessing, which can help you make more deliberate choices while you and your clinician monitor your labs. You can find it here: https://findthe.app/keeto-5m0vbj
Practical Ways to Lower Risk Without Giving Up Keto Benefits
If your LDL rises and you want to stay keto, there are several reasonable adjustments to discuss with a clinician. One option is changing the fat profile. Some evidence suggests that dietary fat type can matter in LMHRs, and shifting away from certain fat patterns may improve LDL without requiring full carb reintroduction. Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC10844582/
Another approach is to look at total calories and energy balance. In some people, chronic under-eating or aggressive weight loss may be part of what drives the lipid rise. Bringing calories closer to maintenance can sometimes reduce LDL and apoB without abandoning ketosis entirely.
You can also review how extreme your carb restriction really needs to be. Some people maintain many keto benefits with a slightly more liberal low-carb intake, especially if their personal goals are metabolic health rather than therapeutic ketosis. For others, modestly increasing carbs from whole-food sources may lower LDL while preserving much of the benefit.
Finally, it is worth revisiting whether the diet is built around lots of saturated fat versus more unsaturated fat and minimally processed foods. Even though saturated fat is not the only driver of LDL on keto, it can still be part of the picture for some people. The best strategy is not one-size-fits-all; it is careful experimentation with follow-up labs.
Questions to Ask Your Doctor About Rising LDL on Keto
If your LDL jumps on keto, useful questions include: What is my apoB, and how does it compare with my LDL-C? What is my non-HDL cholesterol? Do I have Lp(a), familial hypercholesterolemia, or other inherited risk? Should we look at thyroid function, CAC scoring, or repeat labs after a dietary adjustment?
You can also ask how your doctor weighs your other markers. If your triglycerides are very low, HDL is high, blood sugar is improved, and blood pressure is normal, your clinician may interpret the rise differently than if you also have insulin resistance or a family history of premature disease. The point is to build a full risk picture, not to chase one number in isolation.
If your doctor is unfamiliar with LMHR patterns, bringing your own context can help. Explain that you are trying to understand whether the high LDL represents a temporary metabolic response, a marker of particle number that needs addressing, or a sign that keto is not the right long-term strategy for you.
Bottom Line: When Rising LDL Is a Warning Sign, and When It May Need More Context
A rising LDL on keto should always be taken seriously, but not always interpreted in the same way. If LDL rises along with high apoB, adverse family history, existing plaque, or other concerning markers, it is a real warning sign. If LDL rises in a lean, active person with low triglycerides, high HDL, low insulin resistance, and no evidence of plaque, the meaning is more complicated and may require closer follow-up rather than immediate alarm.
The current research suggests that LMHR-type responses are real, relatively common among lean keto dieters, and sometimes dramatic. It also suggests that short-term plaque findings may be less alarming than many people fear. But the long-term cardiovascular story is still unresolved, which is why caution, testing, and individualized decision-making are the right response.
In the end, the goal is not to defend keto at all costs or to demonize LDL blindly. The goal is to understand your own biology. If you monitor intelligently, talk with a clinician who understands lipids, and make targeted dietary changes when needed, you can often keep many of keto’s benefits while reducing unnecessary risk.